|
Introduction of the Symposium Eiji Yano |
|||||||||||||||||||||||||||||||||||||||||||||
|
Contents ■Evaluation and Evidence-based Medicine ■RCT and Cochrane Collaboration ■EBM in British National Health Service ■Okinaga Visiting Professorship Lecture ■EBM and Health in the Population
|
Evaluation and Evidence-based Medicine
In the first Teikyo-Harvard Symposium held in 1994 (1) the importance of evaluation in health and medical care was emphasized. In this present symposium, evaluation turned to be the main theme. Structure of the Symposium (3) The primary mission of this symposium is to comprehend the reality in medical practice that scientific basis of medical technology is insufficient. There we need to consider: what is evidence?, how to create it?, how to access it? The major part of the first day of the symposium was devoted to this point. At first Professor Sackett, the pioneer of this field, from clinical epidemiology to EBM gave the opening lecture on the original concept of EBM. He is the author of the book titled Evidence-based Medicine
(4), and he issues a periodical journal under the same title. His lecture was not only the general overview but also demonstrated the state-of-art of EBM in practice by giving an example performed in the teaching hospital of Oxford University. In the hospital, the Centre for Evidence-based Medicine is housed
(5). RCT and Cochrane Collaboration After the general concept, 'how to get evidence' was discussed. For a clinician, when making a plan for treatment, the traditional way is to collect references and read them carefully and critically. Then, find the best evidence, or information found in the paper(s) with the highest reliability and validity
(6). From this point of view, results form RCT or randomized controlled trial will provide evidence. One may sum up information from several papers by using meta-analysis
(7). RCT, on which the Cochrane Collaboration is based, is performed in an ideal setting using the patients strictly selected to meet the indication of the treatment. The result measured in a RCT is efficacy of the treatment. On the other hand, in a real clinical setting patients may have various conditions other than the target disease, and the treatment itself may not be strictly performed under the required conditions. Hence, the results of the treatment may not be exactly the same as those obtained by RCT. Effectiveness of treatment is affected by many factors such as selection of treatment, appropriateness and timing of the procedure, coordination of the medical personnel and other issues related to process of the treatment
(10). Of course, it is possible to measure the effect of the treatment process by RCT but it may not be clear which part of the process effects to what extent the results. To give the answer to these questions before the intervention study, descriptive study is required and that is why outcome studies under the usual circumstances of treatment are indispensable
(11). Among the many outcome studies launched so far, one of the largest is by Patient Outcomes Research Teams (PORTs)(12). By these outcome studies, it has been revealed that the maneuver of the operator, the general policy of the hospital, coordination of the co-medicals etc. can affect the results of operation. Dr. Barry reported about the outcome studies in the United States by taking prostatic diseases as an example. EBM in British National Health Service Medicine is not only the issue of health and diseases but also the issue of the total life of the patients. Therefore, the results of medicine will be evaluated in the whole life of the patients. Moreover, medicine is not the matter between a doctor and a patient but the matter in the whole society. As a consequence, evaluation of the outcome of medicine will deal beyond the level of the individual patient and to the level of population and society. Prevalence and mortality of the population, life expectancy and proportion of disabled are the examples of the evaluation index at the level beyond the individual. In addition, utilization of hospital beds, medical expenditure per capita and medical expenditure per GNP are other examples of outcomes evaluated in EBM. Okinaga Visiting Professorship Lecture At the end of the first day program of the symposium, Okinaga Visiting Professorship Lecture was given
(14). The Okinaga Visiting Professorship in Harvard 1998 was given to Dr. Shigeaki Hinohara, president of the St Luke's Hospital in Tokyo. It was very timely to have his lecture in the symposium because Dr. Hinohara devoted his life to improve medical practice in Japan and also is one of the pioneers introducing the concept of EBM into Japanese medical society. The second day of the symposium discussed the problems needed to overcome when EBM is applied and performed in making decisions in the actual settings of health and medicine. The areas to apply EBM are: clinical practice, preventive medicine and health policy. At first, Dr. Hashimoto, a Teikyo Faculty who was studying in Harvard summarized the first day discussion and then talked about the limitations of the outcome study. The second afternoon of the symposium was started with the topics of preventive medicine. In Japan, secondary prevention or screening is so widely and extensively performed that preventive medicine is nearly a synonym for health check-ups
(18). However, as Geoffrey Rose pointed out, traditional approach of early detection and treatment by screening (high-risk approach) may overlook the structural factors which decide the fundamental health status of the whole population
(19). The high-risk approach can detect only those deviated within the population but cannot detect the deviation as a whole. On the contrary, the other approach called population approach, deals with the problems of the population. Professor Kay-Tee Khaw who has worked with Rose in the mass survey of WHO on stroke and osteoporosis talked about the population approach in preventive medicine. EBM and Health in the Population The last session of the symposium discussed EBM in health policies and targeted nations and the world. Most effective allocation of the limited resources could be guided by evidences obtained by economic analysis. To measure health in the population and demonstrate it by simple indices is essential for this process. For this purpose, classical indices based on death events such as infant mortality and life expectancy are no longer appropriate to tackle with the current health problems which are characterized by chronic diseases, aging, and highly industrialized society. Recently, new health indices, which take disability into account, have been proposed. Dr. Nonaka gave an overview of them and discussed the longevity and quality of life. Dr. Lopez who developed with Professor Murray the concept of Disability Adjusted Life Years (DALY)(21) talked about it and its potential to assess health problems in nations, regions, and the whole world by quantifying the impact of disease and disability. At the very end of the symposium, Professor Brain summarized the symposium and announced the plan of the fourth symposium, which will discuss aging and health to be held in Boston in the year 2000. As can be seen, this symposium dealt with EBM and the wide variety of dimensions related to health and medical care, starting from clinical practice for an individual patient to the impact of disease in the world. EBM is not merely a concept but a practical strategy that the actual practice is most important. There are a number of obstacles before we can realize EBM and we should not be too optimistic. Therefore, we need to start EBM by evaluating our daily activity in health and medical care. I hope that the symposium and this book can help these activities. (1)
The First Teikyo-Harvard Symposium On
22 and 23, October, 1994 the first Teikyo-Harvard Symposium was held at the
University of United Nations in Tokyo. The theme was "Environment,
Health and Medical Care for the 21st Century." Like the
following symposium, there participated the delegation from Cambridge
University and Oxford University in addition to those of Teikyo University
and Harvard University. There were four sessions regarding health policy,
environment, aging and occupational health. In concluding the first
symposium, the chairman of the symposium emphasized the importance of
evaluation as well as that of prevention, research, education and
coordination for the 21st century.
The report of the first symposium was published from the University
Publisher, Harvard University in 1995 under the same title of the symposium. (2)
Japanese Word for Evidence Based Medicine In
July 1998 in Tokyo, as a preliminary session of the symposium, EBM Forum was
held by having the participation of most of the people who had contributed
to the development of EBM in Japan. The speakers and their titles are listed
in the table. In the forum, the Japanese word for EBM was also discussed but
could not reach an agreement. Rather, we decided to use English word or
Katakana of EBM for a while. The report of the forum will be published in
the Japanese edition of this book.
Table: The speakers and their titles of EBM Forum (July 19, 1998 in Tokyo)
(3)
Structure of the third Teikyo-Harvard Symposium
DL.
Sackett
et al., "Evidence-based Medicine-How to Practice & Teach EBM,"
Churchill Livingstone, 1997. Japanese edition was published by Dr. Testunori
Hisashige from OCC. (5)
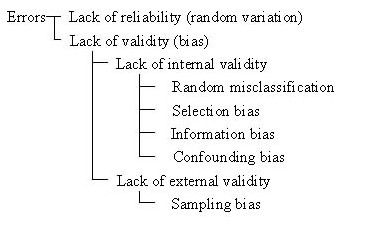
Centre for Evidence-based Medicine One of the world centers, of EBM, housed in John Radcliffe Hospital, a teaching hospital of Oxford University. The first Chairman was Dr. Sackett. It performed research and dissemination of the information related to EBM and also publishes the periodical review journal of "Evidence-Based Medicine." For further information: http://cebm.jr2.ox.ac.uk/ In epidemiological terms, reliability refers to the degree of stability exhibited when a measurement is repeated under identical conditions and validity refers to the degree to which a measurement measures what it purports to measure. Lack of reliability leads to random variation while lack of validity causes bias. Error is a phenomenon when the result of an observation is different from the true value. It is caused either by misclassification or by bias. This can be illustrated by the figure below. Also, the remedy for each cause of error is demonstrated. Table 6-1. Classification of the causes of error
Table 6-2. Examples to prevent or treat errors
A
statistical method of combining the results of several studies with an
identical research question. Instructions
of the clinical procedures which will maximize the efficacy (10). In the
United States many organizations including academic societies, hospitals,
and governmental committees etc. have developed many guidelines. There has
even been a guideline titled “How to use guidelines.” Also in Japan,
Japan Medical Association and medical societies have developed some
guidelines. International collaboration started as a part of British National Health Service in 1992 named after a British physician Professor Archie Cochrane who was the author of “Effectiveness and Efficiency." The collaboration evaluates randomized controlled trials and combines the results by meta-analysis. The summaries of the evaluation and meta-analysis are provided by the internet and CD-ROM. In Japan, headed by Dr. Kiichiro Tsutani (Tokyo Medical Dental University), Japanese Information Network for Cochrane Collaboration (JANCOC) plans to set up Japanese Cochrane Center (JCC). (see:
http://cochrane.umin.ac.jp/) (10)
Efficacy, Effectiveness, and Efficiency A
term used by Donabedian in the model to evaluate quality of medical care. He
analyzed the quality at the levels of structure,
process and outcome. Traditionally objective outcome measures such as
reduction of body temperature for fever, back to the normal range for
abnormal laboratory data, mortality, survival time, complication rate, etc.
have been used. Recently, in addition to the objective measures, subjective
outcome measures of patients such as QOL and patient satisfaction are
getting used. Although there are still criticisms to QOL and other
subjective measures for their lack of clear definition and theoretical
basis, many subjective measures have been used for RCT in the evaluation of
the treatment of hypertension, AIDS and breast cancer, etc. after measuring
their validity and reliability. Because outcome is the result of the
structure and process of medical services, the evaluations for structure and
process are also required. Patient
Outcomes Research Teams (PORTs) is one of the largest ongoing outcome
research projects funded by the American Government in 1990s. There are 14
major diseases specific teams as well as methodology teams such as outcome
measurement, decision analysis etc. The research on coronary bypass
operation in New York City and comparisons among veterans hospitals for
surgical procedures are other examples of major outcome studies.
(13)
Research and Development in National Health Service The Department of Health in Britain emphasized Research & Development (R&D) as an important tool to promote nation’s health. In addition to clinical sciences, sciences for management and policy making are strategically employed to give scientific evidence for political decisions. R&D are practiced both on the national and regional levels. Dr. JA. Muir Gray and Professor Richard L. Himsworth are director and vice director of the Anglia Oxford Regional NHS Office for R&D. See ”Towards an evidence-base for health services, public health and social care”(http://www.open.gov.uk/doh/rdd1.htm). (14) Okinaga Visiting Professorship in Harvard The
Okinaga Visiting Professorship in Harvard started in 1994 under Teikyo-Harvard
Program. Every year, after the recommendation from Teikyo University,
Harvard University nominates both recipients of the Okinaga Visiting
Professorship and the Teikyo-Harvard Prize. Usually the former is invited by
Harvard University to give a lecture and the latter is given to a young
competent scientist.
List
of the intervention procedures to be performed by each medical profession at
each level of clinical process. Also, the items to be checked are listed.
This is used for the standardization of medical care, clarification of
responsibility, increased efficiency and better communication within a
medical team. (16)
Continuous Quality Improvement (CQI) CQI
refers to a continuous quality improvement management system with Plan, DO,
Check and Act (PDCA) cycle. Originally it started in manufacturing
industries and became popular among health organizations in 1980s in the US.
The Total Quality Management (TQM) is a concept of systematic management
strategy with CQI which emphasizes customer satisfaction.
Case
mix refers to a mixture of cases with various characteristics of disease
severity, complication, etc. The difference in these characters affects the
outcome of the medical services that should be controlled before comparison.
Several rating methods for case-mix have been developed and APACHE is one of
its kind to rate the severity of the patients under critical care. (18)
Stages of Preventive Medicine In
1958, Clark & Leavelle proposed the following three stages in preventive
medicine in accordance with the natural history of diseases.
Primary prevention: Health promotion, specific disease prevention such as
immunization etc.
Secondary prevention: Early detection (screening) and early treatment
Tertiary prevention: Limitation of the progression of disability,
rehabilitation In
the book titled The Strategy of Preventive Medicine, G. Rose
contrasted the two strategies in prevention, the high risk strategy and the
population strategy and emphasized the importance of the latter. The former
uses screening, etc. and the latter achieves health promotion by approaching
the whole society with the understanding that health risk exists in the
character of population itself. Translated by Soda and Tanaka, Japanese
edition of this book is published by Igakushoin. (20)
Guide to Clinical Preventive Services A
report of the US Preventive Services Task Force reviewed literatures on the
efficacy and effectiveness of preventive practices such as screening and
health education and gave recommendations. The latest version is the second
edition published in 1996. See http://www.ahcpr.gov/clinic/uspstf.htm.
The first edition was translated into Japanese by Fukui et al, and published
by Igakushoin. (21)
Disability Adjusted Life Years (DALY) A population health index developed by a joint project among WHO, World Bank and Harvard School of Public Health. Christopher JL Murray and Alan D Lopez are the main researchers. DALY quantifies the effects of disease and disability by estimating value reduction from disability, disease and death. See also the major publications by Christopher JL Murray and Alan D Lopez: Lancet. Vol. 349 (1997) May 3, 1269-76; May 10, 1347-52; May 17, 1436-42; May 24, 1498-1504, Global Burden of Disease and Injury Series Vol. 1-Vol. 10 WHO,Harvard School of Public Health, World Bank (http://www.hsph.harvard.edu/organizations/bdu/) |
||||||||||||||||||||||||||||||||||||||||||||
|
[top page]
|
|||||||||||||||||||||||||||||||||||||||||||||